
Coronavirus : Update 15 from the Epicenter
Warning : the widely circulated article on which I based the last section of this post has been partially debunked. Thanks to Simone Naso’s alert in the comments section that points to this in-depth review of the article (in Italian).
The investigation found that the statements in the article came from a private medical forum and were improperly published by persons unknown under a fake name (Prof Giannini). It remarkably concludes that although the article itself should be considered “fake news”, the information in it may prove to be correct..!
I’m therefore going to leave the post up, but please do not treat the last section that refers to the non-existent Professor Giannini as peer reviewed fact. It’s from an anonymous source and at best is a gross-oversimplification of the situation.
Have we finally understood the cause of COVID-19’s lethality?
Why do so many Italian, British, and American patients that enter hospital with severe symptoms never come out, whereas the Germans pop a Bayer Aspirin, go home and recover while watching reruns of the Italia 90 World Cup Final?
Back in Update 9 we looked at the startling difference between the Italian and German outcome curves :
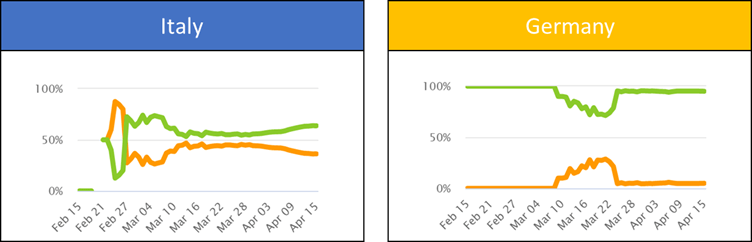
Like everywhere else, Germany suffered an initial surge in deaths, but this quickly died away – as though they knew something that nobody else did.
Fergus Walsh, the BBC’s health correspondent felt he had the answer in this interview :
“It’s because Italians eat pizzas with their fingers and live together in multi-generational households”
…but then the British started dying at an even faster rate than the Italians :

Jair Bolonsaro – Brasil’s president told reporters on March 18th that :
“Italy is a city… a country full of old people. There is at least one couple in every building, like in Copacabana, and that’s why there are so many deaths. They have other diseases, but they say they die from Coronavirus. The Coronavirus that comes at the end does not kill them, those people are already debilitated”
But we saw that the Germans have more-or-less the same median age as Italy.
The most often cited reason however was testing. “Germany is testing more than anyone”. I have a couple of issues with this idea :
Firstly, testing will tend to reduce the ratio between deaths and recovering patients as it changes the size of the denominator. What it doesn’t to is change the absolute numbers dying, which have remained stragely low in Germany :

Secondly, it’s true that Germany has tested more, but not dramatically so : 15.7k / million population compared to Italy’s 14.1k :

Our (crappy) working hypothesis was a mix of three factors :
- Despite the cruelty of his tone, Bolonsaro may have been partially correct. The factor separating different geographical death rates in Italy appeared to be whether or not COVID-19 had hit a region’s elderly care homes. The median age of Italian patients was 20 years older than German infected population.
- The Germans are fudging their numbers – reporting COVID-19 deaths as pneumonia. In order to understand if this is true we would need to see the total deaths in March and April and compare them to seasonal averages.
- The German healthcare system has more than double Italy’s ICU beds per capita, and there was capacity to spare, whereas Italian doctors were having to triage patients and decide which ones would get an incubator. This didn’t explain why so many would go on to die in the US, however – even though they had an excess of critical care beds :

However, a recent article that interviews a professor at the heart of Italy’s emergency response provides a new possible explanation :
People are dying in our ICUs because they have pulmonary thromboses [blood clots in their lungs]. In this case, resuscitations and intubations are useless because first of all you have to dissolve, or rather prevent these thromboembolisms. If you ventilate a lung where the blood doesn’t arrive, it’s no use. Indeed 8 out of 10 patients in this situation die. The problem is cardiovascular, not respiratory. It’s venous microthrombosis, not pneumonia that causes the fatality.
Professor Sandro Giannini of the Rizzoli Clinic in Bologna
In Update 12 we explained that the severe cases are caused by the inflammatory response to the virus :
Part of the innate immune response is to cause ‘inflammation’. That is useful in containing the virus early in an infection but can result in widespread damage of uninfected tissue (we call this a ‘bystander effect’) if it becomes too large and uncontrolled, a situation named ‘cytokine storm’. It is difficult to manage clinically, requiring intensive care and treatment and carries with it high risk of death.
http://www.orchard.it/coronavirus-update-12-from-the-epicenter/
Professor Giannini suggests that the inflammation causes clots that stop the blood getting to the lungs, rendering incubators useless.
You can find the link between inflammation and vascular clotting in school textbooks, so why didn’t this explanation come to light before? The Professor provides two reasons :
- The clots are tiny “microembolisms” that don’t show up on the scans
- The official advice coming out of China was to avoid the use of Anti-inflammatory drugs during COVID-19 treatment
Professor Giannini wondered why, despite their age, no patient with rheumatoid arthritis had been admitted into the Rizzoli ICU since the epidemic started :
Patients with arthritis do not get severe COVID symptoms because they use cortisone, a powerful anti-inflammatory. If we treat other patients in this way then COVID-19 becomes something we can handle successfully at home. No more epidemic.
Why the Chinese were advising against the use of these cheap and widely available drugs is unclear. We know that the UK and US have also been following this advice, and their situation has mirrored that of Italy.
If this hypothesis proves to be correct… then I’d like to know if this somehow explains Germany’s miracle numbers. Have they been bucking the trend and treating COVID-19 with anti-inflammatory drugs? If so, why has news of their approach not been made more widely available?
Watch this space to see how the story unfolds…
The statement attributed to professor Giannini maybe correct, but nobody knows who actually said it (see here: https://tinyurl.com/y7bw2hyn).
A couple of points:
1. in the complete “Giannini’s post” not all the anti-inflammatory drugs are considered good, only the ones that inhibit the COX-2 but not the COX-1 are OK (https://it.wikipedia.org/wiki/Inibitori_selettivi_della_COX-2) , maybe this is partially recovering Chinese physicians…
2. what seems to work is heparin, not only for prevention, but also as a cure. Aspirin has anticoagulant effect, maybe this is the reason why it works?
Thanks Simone. You are my official fact checker!
This is fascinating. The long article you reference calls Giannini’s statement “fake news, but possibly correct”
What!?!
I will edit the post tomorrow to reflect this bizarre development.
As to your second point, my mention of Bauer Aspirin was more of a cultural reference and not an indication that it is really curing Germans.
Median age, capacity of ICUs and testing rate, all of them explain Italy/Spain vs. Germany. Not Japan vs. Germany though. Japan might be still waiting for the worst to come.
Instead, India is puzzling, unless it’s about the reliability of their data collection and reporting.
Thanks for the comment Suha. Median age is the same, although median infected age is higher in Italy.
Testing rates are in the same ballpark (despite the headlines), and I don’t understand what a few additional tests does to radically improve death rates; percentage of cases dying yes, but absolute numbers, no.
I also don’t see why ICU availability is so important. In Italy if you enter the ICU you don’t come out. In Germany fewer enter and more exit.
I agree that India is surely a reporting issue, although infection (even inside Italy or the US) is far from even. Something is going on, and that’s what I’ll try to examine in the next Update.